



EDUCATION
Residency training and clinical and research fellowships at Stanford in Retina, Glaucoma, Cornea, Oculoplastics, Pediatrics and Neuro-Ophthalmology, as well as special fellowships in international health and ophthalmic innovation, together offer exciting opportunities to advance the field and develop careers.
WELCOME

Jeffrey L. Goldberg, MD, PhD
Professor and Chairman
Department of Ophthalmology
Welcome to the Byers Eye Institute in the Department of Ophthalmology, at Stanford University School of Medicine, a top-tier, internationally recognized, multidisciplinary center combining world-class resources with a commitment to providing the highest level of diagnostic and therapeutic care to our patients.
Through an integrated, personalized approach to healthcare delivery, our dedicated team provides the latest therapies in treating eye disorders. Associated with Stanford Health Care, and the Lucille-Packard Children's Hospital, our faculty and staff provide excellence in ocular and vision healthcare to patients across Northern California and from around the world, while our cutting-edge team of researchers carries out some of the most innovative laboratory research and clinical trials anywhere.
Whether you are a patient, a resident, or a leader in academic or clinical ophthalmology, I invite you to explore our programs, visit our clinics and operating rooms, and receive your eye care from our premier faculty.
I am very proud of our exceptional faculty and staff and their accomplishments in our mission areas of patient care, research, education and community outreach.
We are here for you.

FACULTY RECRUITMENT

We are searching for the best clinicians, clinician-scientists, and vision research scientists to join our faculty at Stanford. If you are looking for staff positions in administration or laboratory or clinical research, please follow this link.
In the News

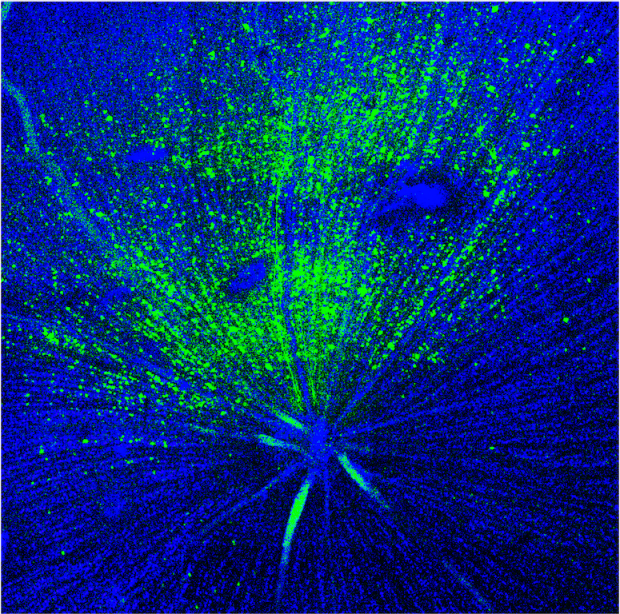
A new avenue for treating neurodegeneration, injury
Jeffrey Goldberg, MD, PhD, is working on a young, underexplored class of therapies called gliotherapeutics, which target and harness glia and will ultimately provide important new directions for treatment, he told Stanford Medicine last month.
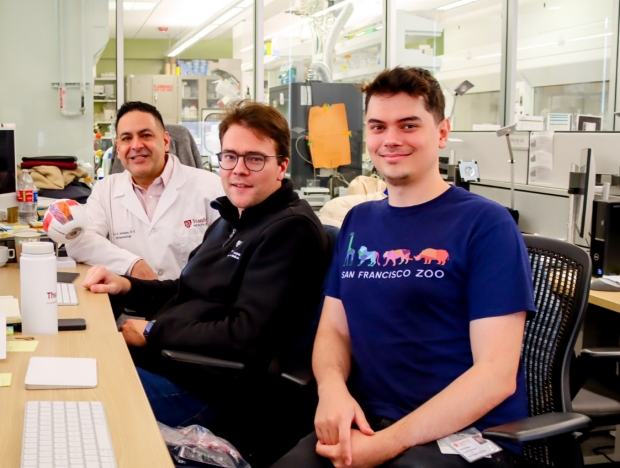
Stanford researchers build an eye ‘aging clock’
Vinit Mahajan, MD, PhD, professor of ophthalmology and Julian Wolf, MS, a postdoctoral researcher in Mahajan's lab, published a groundbreaking paper in Cell describing how to measure ocular aging and identify how disease.

Using video games to measure the eye-brain-body connection
Stanford Medicine published a story on Byers Eye Institute's Khizer Khaderi, MD, MPH, who is working on showing how video games could give ophthalmologists an easy window into eye health and the eye-brain-body connection.

Stanford Medicine launches "I Am Human" campaign
Stanford Medicine launched its "I am Human" campaign, aiming to shift healthcare culture toward vulnerability, self-compassion, community, and connection. The launch video features Jeffrey Goldberg, MD, PhD, chair of ophthalmology at Stanford.

Listen Now: Dr. Jeffrey Goldberg, chair of Ophthalmology at Stanford, on the Huberman Podcast
Learn about eye care at all ages — from infant to adult and as we age — as well as the latest in research to protect and improve our vision, and exciting initiatives at the Byers Eye Institute.

Mid-year check-in with Dr. Jeffrey Goldberg, Chair of Ophthalmology at Stanford
During Dr. Goldberg's tenure as chair, the team at the Byers Eye Institute has grown significantly.
The Stanford Ophthalmology 2023 Annual Report highlights the department's recent news and accomplishments
The recent issue of Stanford Medicine magazine, a theme issue on eyes and vision, includes details about projects and others pushing the boundaries of biology and technology to help people see. Click here to learn more
Illustration by John Hersey